| TOE - Longitudinal views |
Longitudinal views are obtained at the same levels as transverse
ones, that is:
Detailed longitudinal images should be obtained at these levels.
Important views are:
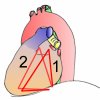
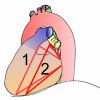
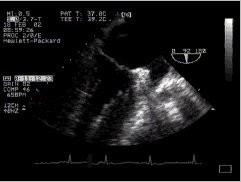
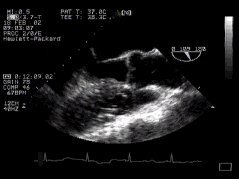
The transgastric two-chamber view is of value in assessing the left atrium, left ventricle, the medial scallop of the posterior mitral leaflet and lateral segment of the anterior mitral leaflet, asynergy of the anterior and posterior walls of the left ventricle, and (occasionally) visualisation of the LVOT.
The anterior mitral leaflet (aml) is well seen, as well as the left ventricular and atrial chambers. The inferobasal portion of the left ventricle is particularly well seen in this view - perhaps the major justification for this particular part of the TOE examination! (The inferobasal part is that part of the LV in the upper portion of the image, close to the probe). Remember that in the visible human from which these anatomical sections were taken, the left side is particularly poorly filled, and thus the LV cavity appears much plumper in the echo image. Compare the above with the two-chamber mid-oesophageal view.
The anatomical section shows the LV cavity, left ventricular outflow tract (lvot), and anterior leaflet of the mitral valve (aml) rather well.
This view provides an excellent four chamber perspective, and good
views of the aortic valve. It is tricky to obtain
(and particularly uncomfortable in the awake patient) but may provide valuable
information.
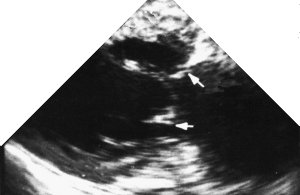
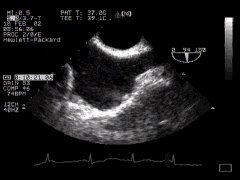
B. Mid-oesophageal viewsThe mid-oesophageal two-chamber view is useful in visualisation of the left atrial appendage (as well as the LA and LV), the middle scallop of the PML, the lateral segment of the AML, and abnormal wall motion in the posterior, anterior and apical LV. PitfallsThe ridges of the pectinate muscles in the left atrial appendage are sometimes interpreted as "clots". One must also be careful to distinguish the LAA from the left upper pulmonary vein! If fluid is present in the oblique sinus around the LAA, this may be falsely interpreted as the LAA! In addition the junction of the LA and LUPV is so often mis-interpreted as being a thrombus that this has been nicknamed the "warfarin ridge"!
The left ventricular cavity and mitral valve are well seen. "Fine tuning" by careful probe movement can be used to demonstrate the papillary muscles and details of the mitral valve leaflets. (Inferior papillary muscle on your left, anterior on the right).
The left atrial appendage is important. Here you can see that it often has coarse trabeculation, and in addition the junction of the left upper pulmonary vein and left atrium close to the LAA can give a mass-like effect.
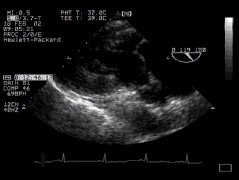
The following view is sub-optimal, as the view of the ventricle is somewhat oblique, and the aortic valve isn't well seen. C. Basal views
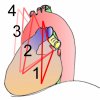
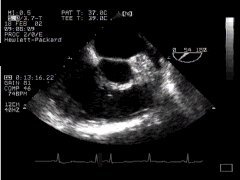
In the basal longitudinal plane views, a host of structures can be seen if one rotates the probe from left (counter-clockwise) to extreme right (clockwise). As we rotate the probe from the left, these are in turn:
The atrial septal view is particularly good for visualising shunts (together with echocardiographic contrast administration i.e. saline with microbubbles). PitfallsA prominent Eustachian valve can resemble a mass in the right atrium. Similarly, the point of junction of the right atrium and superior vena cava can be falsely interpreted as a "mass".
Not only the left upper pulmonary vein (lupv) can be seen, but the left atrial appendage (laa) and the prominent area of tissue between, often mis-identified as thrombus (the warfarin ridge, wr)! In the anatomical section, the mitral valve and left ventricle are rather poorly visualised.
The right ventricular outflow tract is well shown here, and can be followed on the right up to the main pulmonary artery. Closer to the probe is the aortic valve, just beginning to appear as the left ventricular outflow tract leads into it, and closer still (more posterior) the left atrium.
The aortic root is seen in long axis. Gentle repositioning of the probe will also demonstrate the aortic leaflets in profile.
In these images, the superior vena cava (svc) is on the right and inferior vena cava on your left as you view them. This is the so-called "bicaval view"! At the top of the screen near the probe is the left atrium. Adjacent to the left atrium (on your right) you can see the right pulmonary artery.
The right upper pulmonary vein can be seen in continuity with the left atrium. The inferior vena cava (ivc) can just be seen on the left, peeking into the picture. It may be possible to also view the right atrium in this view, but we couldn't achieve this on the visible human!
The anatomical image is far from perfect - the left ventricular outflow, aorta and aortic valve can be visualised, but the left ventricle is foreshortened. Far from the probe at the bottom of the picture, the right ventricular outflow is also seen. |






















| < Previous | ^ Home | Next > |