The following chest x-ray and ECG are of a twenty-five year old
woman, who presented with worsening dyspnoea. She was still on
warfarin anticoagulation following a large pulmonary embolus one
year previously. Despite extensive work-up, there was no evidence
of underlying thrombophilia, and Doppler ultrasound of both lower
extremities had shown no evidence of venous thrombosis. Now, at this visit,
the woman had markedly limited effort tolerance.

Fig 1. Chest x-ray of the patient
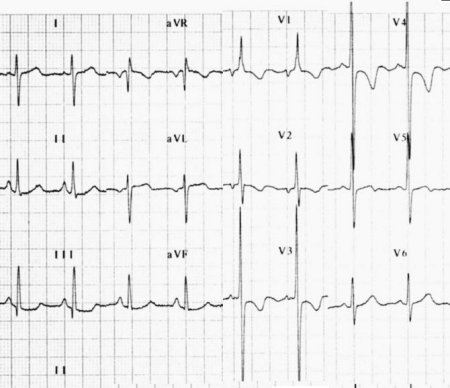
Fig 2. ECG showing right axis deviation, 'P pulmonale',
and
evidence of right ventricular hypertrophy.
Echocardiogram revealed right ventricular hypertrophy, and showed a sytolic pulmonary artery pressure of 106 mmHg. A ventilation scan was normal, but the perfusion scan was as follows:
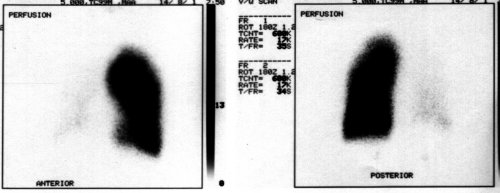
Fig 3. Tc-99m isotope perfusion scan
Surgical Intervention!
The appropriate intervention is pulmonary thromboendarterectomy . This is non-trivial surgery, and should probably still be restricted to the relatively few institutions (and surgeons) with the relevant expertise. In the best centres (UCSD) the peri-operative mortality is now under 9%, a significant figure, but still far better than relegating such patients to the ratbag of medical therapy. A recent report on 273 consecutive patients [Am J Respir Crit Care Med 1996 153 A92 {abstr}] gives an in-hospital mortality of 6.6%.
Pre-operative work-up should include echocardiography, ventilation-perfusion scanning, and pulmonary angiography. Note that large pulmonary artery thrombi may be found in patients with pulmonary hypertension (presumed to be primary) without segmental or larger defects on perfusion scan. Such thrombi are thought not to be haemodynamically significant, and thromboendarterectomy in such cases is probably of no value [Circulation 1995 Feb 1;91(3):741-5] ! However, if there are segmental perfusion defects, then the severity of the perfusion defect correlates poorly with haemodynamic compromise, according to an earlier article from the same group [Chest 1988 Jun;93(6):1180-5] - rather confusing, really.
Criteria for surgical selection
Fairly well-defined criteria exist:
- Thrombi must be accessible (defined by angiography/angioscopy) - endarterectomy is feasible only for chronic thrombi whose proximal location extends to the main and lobar arteries. Total removal of such thrombi must be the goal. Extensive small vessel (segmental) disease correlates with poor outcome.
- The vascular obstruction must be causing haemodynamic or ventilatory impairment. Most patients have effort intolerance, and raised pulmonary vascular resistance (over 300 dyn.s.cm -5 ) is almost the rule, especially with exercise. Surgery is probably indicated even with moderate degrees of pulmonary hypertension at rest, if pulmonary arterial pressures soar with mild exercise.
- Severe co-morbid conditions (such as severe parenchymal lung disease) should be absent, as these have a substantial negative effect on outcome. Age on its own does not appear to be a contra-indication, up to the age of eighty years.
- The patient must be prepared to accept the significant risk of peri-operative death.
Surgical treatment involves deep hypothermic arrest, with complete removal of all thrombus from affected branches of the pulmonary arteries. Failure of surgery to correct the pulmonary hypertension is usually related to inadequate surgery, or recurrent thromboembolism. (It has also been suggested that post-operative outcome is better with avoidance of inotropes, vasodilators and high tidal volume ventilation, to limit reperfusion injury and possibly mortality [Anesth Analg 2000 Feb;90(2):267-73], but the design of the study doesn't allow us to distinguish the effects of these three variables).
Alternative surgical strategies have been described that avoid the need for deep hypothermic arrest, but these have not been validated on large numbers of patients. Another possible curative surgical therapy for pulmonary hypertension is of course lung transplantation (or combined heart and lung transplantation), but this necessitates lifelong immune suppression, with substantial risks of opportunistic infection, and a 30% risk of bronchiolitis obliterans and rejection. For balloon angioplasty in those not amenable to surgery, see [ Circulation 2001 Jan 2;103(1):10-3].
Surgical Outcomes
As already mentioned, adequate surgery is usually curative. Six(+) year survival is reported by the UCSD group to be over 75% [Archibald et al, Am J Respir Crit Care Med 1999 160 523-8], although the nature of their survey (a postal questionnaire with a response rate of 73%) may have introduced bias - this is well-discussed by the authors. Ninety-three percent of the patients in the survey reported a New York Heart Association functional class of one or two. Many patients previously unable to work or live normal lifestyles reported a return to normal levels of activity.
There are several caveats:
- Patients must be on lifelong anticoagulation;
- At UCSD it is apparently routine practice to insert a filter in the inferior vena cava to prevent recurrent emboli.
Apart from the risk of intra-operative mortality, there is a significant incidence of post-operative complications in ICU. One that has received some prominence (especially in cases such as the above one, with markedly diminished blood flow to one lung), is the risk of reperfusion injury to the lung.
Unresolved Questions
'CTEPH' seems to be a decidedly uncommon disorder (although we are sure that every year, thousands of patients die worldwide because they are denied surgery for the condition). Why should these patients not lyse their clots like other individuals?
- Lang et al looked at the endothelial cell-associated fibrinolytic system [Circulation 1994 Aug;90(2):706-12]. In 13 patients endothelial TPA levels and and PAI-1 were no different from controls, and the response to thrombin was normal.
- Welsh et al [Chest 1996 Sep;110(3):710-7] report impaired fibrinolytic activity associated with chronic pulmonary hypertension.
- Altman et al [Clin Cardiol 1996 Jul;19(7):549-54] implicate increased PAI-1 levels in the impaired fibrinolysis they observed (together with a prolonged euglobulin clot lysis time).
- Huber et al [Am J Respir Crit Care Med 1994 Oct;150(4):929-33] also report diminished fibrinolysis.
- See [Blood Coagul Fibrinolysis 1998 Mar;9(2):107-17] for a more recent review on altered haemostasis in pulmonary hypertension.
- A Japanese abstract [Nippon Rinsho 2001 Jun;59(6):1053-8] indicates that patients with pulmonary arterial hypertension have high plasma levels of soluble P-selectin, and low thrombomodulin.
Severity of pulmonary hypertension may not relate to the size of the thrombus - other factors may be responsible. Consider [Am J Respir Crit Care Med 2001 Jul 15;164(2):319-24] implicating Monocyte chemoattractant protein-1 (MCP-1), but is this cause or effect? Likewise for human angiopoietic gene expression (angiopoietin-1) [J Thorac Cardiovasc Surg 2001 Jul;122(1):65-73].
We would also be most interested in reports on the thromboelastogram in such patients.
Footnote
The patient briefly discussed above did well following pulmonary thrombo-endarterectomy. No reperfusion injury was seen, and pulmonary artery pressures dropped dramatically. (Parenthetically, we note that the surgery in this patient was performed in a third-world country by a surgeon with significant expertise in the operation. Ideally, such cases should of course be referred overseas to institutions with considerable experience in the surgical and peri-operative management of chronic thromboembolic pulmonary hypertension, but cost then becomes a major, and often prohibitive issue).